Hemorrhagic Renal Cyst
In 1 minute
A hemorrhagic renal cyst usually appears as a well-defined, homogeneous, hyperdense renal lesion on non-contrast CT because blood products raise its attenuation.4 This is why it can look worrisome at first glance and be confused with a renal tumor. In the Bosniak 2019 framework, a homogeneous renal mass measuring 70 HU or more on non-contrast CT is highly likely to be a benign hyperattenuating cyst.1
The key radiology question is not just "is it dense?" but "does it truly enhance after contrast?" A lesion that remains nonenhancing supports hemorrhagic renal cyst, while real enhancement raises concern for a cystic renal neoplasm such as RCC. On CT, an attenuation change of 10 HU or less is usually treated as nonenhancing, more than 20 HU supports enhancement, and 10-20 HU is equivocal.1 Under Bosniak v2019, a homogeneous nonenhancing hyperattenuating cyst is Bosniak II regardless of size, which matters because older size-based habits often escalated these lesions more than necessary.113
Fast engineer rule: high HU alone does not mean tumor. Think hemorrhagic renal cyst when the lesion is homogeneous, well-defined, hyperdense on non-contrast CT, and shows no true enhancement, no enhancing septa or nodules, and no obvious heterogeneity.117 Be cautious when there is real enhancement, a thickened enhancing wall or septa, a mural nodule, or other suspicious heterogeneous components.23
Quick diagnostic logic
| Situation | What radiologists look for | Why it matters |
|---|---|---|
| Ultrasound finds a cystic renal lesion | Simple versus indeterminate appearance | Ultrasound is good for spotting a cyst, but indeterminate lesions usually need CT or MRI characterization |
| Unenhanced CT shows a homogeneous hyperattenuating cystic lesion117 | Whether attenuation is around 70 HU or greater and whether the lesion is smooth and homogeneous | A homogeneous lesion in this range strongly favors a benign hyperattenuating, often hemorrhagic, cyst |
| Postcontrast CT appears to show slight enhancement116 | Whether the change is true enhancement or pseudoenhancement, especially in a small endophytic cyst next to avidly enhancing parenchyma | CT can overcall enhancement in exactly the lesions that are hardest to characterize |
| MRI shows T1-bright cyst content31014 | Whether the lesion is homogeneous and markedly T1 bright with smooth borders versus heterogeneous or irregular | Diffuse marked homogeneous T1 hyperintensity strongly favors hemorrhagic cyst, while heterogeneous T1-bright lesions can still hide papillary RCC |
| Postcontrast CT or MRI shows enhancing wall, septa, or nodule23 | Enhancement pattern and Bosniak complexity | Enhancement raises concern for cystic renal neoplasm rather than a benign hemorrhagic cyst |
Example figures
These examples are lesion-specific hemorrhagic renal cyst figures rather than generic Bosniak comparison images. The first two are embedded because the source article is open access under CC BY 4.0 and the figure annotations explicitly point to the hemorrhagic cyst.11
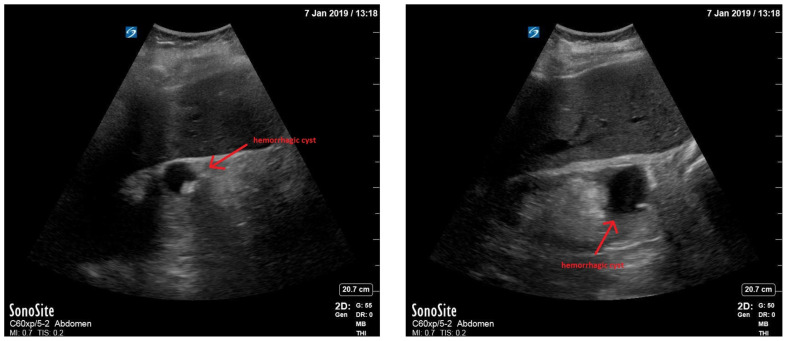
Figure 1. Bedside renal ultrasound from a hemorrhagic renal cyst case report. The source article describes the internal echogenic debris and red-arrow target as findings consistent with a hemorrhagic cyst, which makes this a useful ultrasound example of why a benign cyst can stop looking simple. Source:
Rometti et al., Figure 1
, CC BY 4.0.11
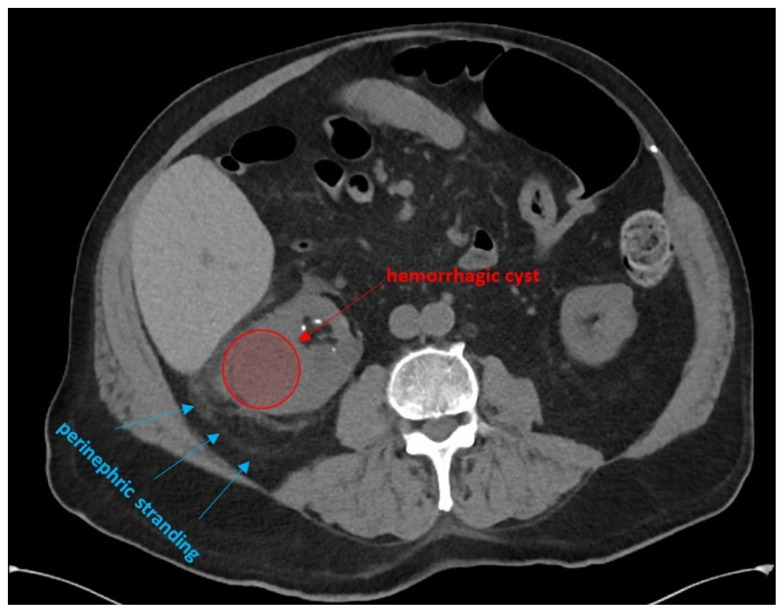
Figure 2. CT from the same case report, where the article says the scan confirmed a right renal cyst with mild perinephric stranding possibly consistent with a hemorrhagic cyst. This is a lesion-specific CT example, but it is still a case-report confirmation image rather than a full renal-mass-protocol teaching series. Source:
Rometti et al., Figure 2
, CC BY 4.0.11
Additional lesion-specific figure links:
- MRI example of a small hemorrhagic renal cyst communicating with a perinephric hematoma in a more unusual case: See original Figure 2.12
- Ultrasound example from the same unusual case, where the hemorrhagic cyst is shown communicating with the perinephric hematoma: See original Figure 3.12
Common confusions
- Simple renal cyst: thin-walled, fluid-filled, and typically straightforward
- Hemorrhagic or proteinaceous cyst: still often benign, but denser or brighter on some sequences because of internal contents
- Bosniak II or IIF cyst: a structured way to describe mildly more complex cystic lesions; the cyst can be hemorrhagic, but the Bosniak class is a separate structure-plus-enhancement judgment
- Cystic RCC: suspicious because of enhancing soft tissue, nodularity, or more worrisome complexity
Engineer-first takeaway
If you only remember one thing, remember this: a hemorrhagic renal cyst is not automatically a tumor, and a single high-HU non-contrast image is not enough to call it suspicious. From an engineering and informatics perspective, the important workflow is to preserve the phase context and compare non-contrast and post-contrast behavior rather than reacting to density alone.
If you build search, NLP, or label-normalization pipelines, it is useful to keep nearby report terms linked rather than isolated. Useful related terms include:
- hemorrhagic renal cyst
- hyperdense cyst
- proteinaceous cyst
- complex renal cyst
- Bosniak cyst
- cystic renal mass
This concept also maps naturally to technical tasks such as:
- classification: benign-appearing cyst versus suspicious cystic renal mass
- segmentation: kidney and lesion delineation on CT or MRI
- report understanding: extracting Bosniak class, enhancement language, and follow-up recommendations from narrative reports
There is no clean public benchmark specifically labeled for hemorrhagic renal cyst. Public renal-mass datasets are still useful starting points, but they should be treated as partial proxies rather than lesion-specific ground truth. In practice, the closest public resources are broader renal-mass or kidney-plus-cyst datasets, especially when multiphase CT is available for enhancement logic.768
Related research map
Cystic workup cloud
Foundational and problem-solving papers for deciding when a complex cyst still behaves like a benign hemorrhagic lesion.
Engineering and data cloud
Review and dataset papers that matter once the question shifts from diagnosis alone to labels, phases, benchmark honesty, and model design.
Narrow MRI mimic cloud
Focused MRI papers for the T1-bright hemorrhagic cyst versus RCC question that often drives escalation.
2023
KiTS23
Good for kidney, tumor, and cyst segmentation, but still broader than a hemorrhagic-cyst-only benchmark and weak on lesion-specific cyst semantics.
2024
UCSF RMaC
Especially valuable because multiphase CT is closer to the real engineering task of measuring baseline density versus enhancement, even though the labels are still broader than hemorrhagic cyst alone.
Clinical and pathology background
A hemorrhagic renal cyst is best thought of as a renal cyst complicated by intracystic bleeding. Once blood products accumulate, the lesion stops behaving like simple fluid: attenuation rises on unenhanced CT, MRI signal can become T1 bright, and the cyst may look more complex than a simple benign cyst.24 Hemorrhage or infection can also increase cyst size, attenuation, or wall enhancement, which is one reason these lesions can look unsettling in real practice.4
The deeper clinical framework is the Bosniak classification for cystic renal masses, which is built around structure plus enhancement rather than density alone. Smooth, homogeneous, nonenhancing hyperattenuating cysts usually stay in a benign category, whereas measurable enhancement, irregular or thickened wall/septa, and enhancing nodules move the lesion toward Bosniak III or IV and stronger concern for cystic renal neoplasm.12 This is why a dense lesion on one phase can still be benign, but a dense lesion with true enhancement is a different problem.
MRI is often the problem-solving study when CT remains indeterminate. Bosniak v2019 highlights that some masses with T1-hyperintense contents can still represent papillary RCC, while MRI subtraction can uncover enhancing nodules that CT attenuation measurements may miss.3 In the opposite direction, diffuse marked T1 hyperintensity strongly favors hemorrhagic cyst, and CT can be confounded by pseudoenhancement in small endophytic cysts near avidly enhancing renal parenchyma.31016 So the practical background is not just "blood in a cyst"; it is an overlap pattern where phase behavior, enhancement assessment, and modality limitations determine whether the lesion stays benign or becomes suspicious.
Management should be described as Bosniak- and symptom-based, not as routine serial ultrasound for every hemorrhagic cyst. Bosniak I and II lesions do not need routine follow-up, Bosniak IIF lesions are followed at 6-12 months, then yearly for 5 years if stable, and symptomatic cysts can be treated for pain, bleeding, infection, or obstruction regardless of whether the imaging goal is otherwise complete.13 Once the lesion moves into Bosniak III or IV territory, the discussion is no longer really about a benign hemorrhagic cyst alone, because enhancement and nodularity reopen the cystic neoplasm pathway.131
Scope and caution
This page is educational and intentionally simplified for technical readers. It does not replace formal radiology interpretation, urology evaluation, local policy, or patient-specific medical advice.
References
- Bosniak Classification of Cystic Renal Masses, Version 2019: https://pmc.ncbi.nlm.nih.gov/articles/PMC6677285/
- CT and MR imaging of cystic renal lesions: https://pmc.ncbi.nlm.nih.gov/articles/PMC6942066/
- Update on MRI of cystic renal masses including Bosniak version 2019: https://pmc.ncbi.nlm.nih.gov/articles/PMC8017011/
- Renal cysts and urinomas review: https://pmc.ncbi.nlm.nih.gov/articles/PMC3312170/
- Automatic Segmentation of the Kidneys and Kidney Tumors: The KiTS19 International Challenge: https://pmc.ncbi.nlm.nih.gov/articles/PMC8763784/
- KiTS23 challenge: https://kits-challenge.org/kits23/
- UCSF RMaC: University of California San Francisco 3D Multi-Phase Renal Mass CT Dataset with Tumor Segmentations: https://pubmed.ncbi.nlm.nih.gov/41728332/
- Artificial intelligence and radiomics in evaluation of kidney lesions: a comprehensive literature review: https://pmc.ncbi.nlm.nih.gov/articles/PMC10126666/
- Cystic renal mass screening: machine-learning-based radiomics on unenhanced computed tomography: https://pubmed.ncbi.nlm.nih.gov/38164893/
- Visual Assessment of the Intensity and Pattern of T1 Hyperintensity on MRI to Differentiate Hemorrhagic Renal Cysts From Renal Cell Carcinoma: https://pubmed.ncbi.nlm.nih.gov/27845847/
- Hemorrhagic Renal Cyst, a Case Report: https://pmc.ncbi.nlm.nih.gov/articles/PMC10332543/
- A Renal Colic Mimic - Wunderlich Syndrome: A Case Report: https://pmc.ncbi.nlm.nih.gov/articles/PMC7707131/
- 2023 UPDATE – Canadian Urological Association guideline: Management of cystic renal lesions: https://pmc.ncbi.nlm.nih.gov/articles/PMC10263289/
- Homogeneous T1 Hyperintense Renal Lesions with Smooth Borders: Is Contrast-enhanced MR Imaging Needed?: https://doi.org/10.1148/radiol.16151240
- Are Hemorrhagic Cysts Hyperintense Enough on T1-Weighted MRI to Be Distinguished From Renal Cell Carcinomas? A Retrospective Analysis of 204 Patients: https://doi.org/10.2214/AJR.19.21257
- In Vivo Predictors of Renal Cyst Pseudoenhancement at 120 kVp: https://pmc.ncbi.nlm.nih.gov/articles/PMC4328313/
- Can high-attenuation renal cysts be differentiated from renal cell carcinoma at unenhanced CT?: https://doi.org/10.1148/radiol.2432060559